


It was October 2012. I had been invited to give a lecture on secondhand drinking (the negative impacts of a person's drinking behaviors on others) to Stanford Medical School students enrolled in Dr. Stanley Fischman's Eating Disorders and Addiction Rotation.
Dr. Fischman asked me to speak with his rotation students on a regular basis given my decades experience with loved ones' alcohol misuse, my own eating disorders, and my relevant work experience. He wanted his students to understand the other side of a person’s alcohol misuse – secondhand drinking (SHD) – because it affects 90 million Americans. That’s five times the number of people whose drinking causes SHD, yet medical practices are primarily focused on the drinker and the health impacts the drinker experiences.
During my lecture, I explained drinking behaviors, which are at the root of SHD. Drinking behaviors occur when a person consumes more alcohol, thus more ethyl alcohol chemicals, than their liver can metabolize. When this happens, the ethyl alcohol chemicals interrupt the chemical portion of the brain's cell-to-cell communications. This suppresses normal neural network functioning responsible for judgment, memory, pleasure/reward, emotions, breathing.... In other words, it changes a person's thoughts, feelings, and behaviors.
Contrary to popular belief, it's not just the drinking pattern of alcoholism that causes these behavioral changes, although alcoholism is certainly one. Binge drinking, heavy social drinking, and alcohol abuse (terms now grouped together as alcohol misuse and/or alcohol use disorders) also cause drinking behaviors. Some of the drinking behaviors I referenced included:
- crazy, convoluted accusations and illogical arguments
- verbal, physical and/or emotional abuse
- bullying; neglect
- driving while impaired
- domestic violence.
I went on to explain there is a direct impact – a second-hand effect – on people confronted and/or coping with those drinking behaviors. These include:
- being on the receiving end of drinking-related verbal, physical or emotional abuse; neglect; bullying and believing it’s the “real” person coming out, not understanding the behaviors are the consequence of chemical changes in the brain
- being seriously injured by an impaired driver
- feelings of anxiousness, hopelessness, walking on egg shells because of the uncertainty, worry, fear, anger, concern triggered when in the sphere of an impaired person’s drinking behaviors
- being on the receiving end of domestic violence or a sexual assault by a person whose brain functioning has changed under the influence of alcohol.
For the moms, dads, husbands, wives, brothers, sisters, children, grandchildren, grandparents, boyfriends, and girlfriends directly exposed to SHD, coping with these sorts of drinking behaviors activates their stress response. When this system is repeatedly activated, their stress becomes toxic, and they experience many of the following stress-related symptoms:
- stomach ailments
- insomnia
- anxiety, depression, frequent or wild mood swings
- chronic neck and/or shoulder pain
- frequent headaches, migraines
- chest pain, palpitations, rapid pulse
- increased anger, frustration, hostility
- feeling overloaded, overwhelmed, helpless, hopeless
Screening for Alcohol Misuse in the Family is Screening for SHD and ACEs
During the lecture I referenced above, a student asked if I thought it was appropriate for a physician to ask a patient about drinking patterns of family members when the patient presents with stomach ailments, migraines, anxiety, depression, skin rashes, unexplained joint pain….
My unequivocal answer was "YES!" I would have given anything if my doctor had asked me about alcohol misuse in my family when I went in to talk with her about feeling depressed. Not my drinking, but that of my family members.
Instead, I was diagnosed with situational depression and put on Prozac for several months. When that didn't seem to work, I was put on Zoloft. That didn't work, either. I wasn't "depressed," but I wasn't "living" either.
Given 90 million Americans are affected by secondhand drinking, I continued, not screening for alcohol misuse in the family when presented with a patient exhibiting stress-related symptoms is to miss a powerful opportunity to help millions of Americans improve their lives and their life-long health.
Why? How? Because of the ACEs—SHD connection.
Both ACEs and SHD cause toxic stress because of their chronic activation of the stress response system. Toxic stress results in the stress-related symptoms named above.
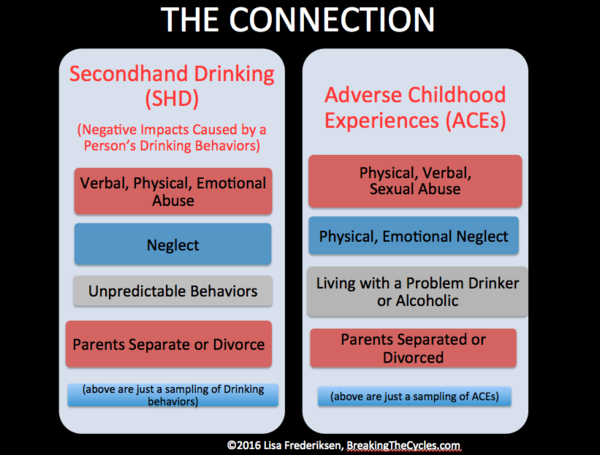
One of the ACEs measured in the ACE study was living with a problem drinker or alcoholic. In other words, someone whose drinking causes drinking behaviors. Drinking behaviors cause negative impacts. Four examples of SHD – the negative impacts of a person’s drinking behaviors on others – listed in the left SHD column above are identical to three of the ACEs listed in the right ACEs column above.
Continuing with my response to the medical school student…
Had my physician screened for family alcohol misuse by asking the following screening question:
How many times in the past year has someone in your family or someone with whom you are in a close relationship had 4 or more standard drinks on any day (for women) or 5 or more standard drinks on any day (for men)?
the floodgates would have opened.
I would have poured forth the pain and confusion and concerns and fear and repeated attempts to make the drinking stop and shared the insanity of what it was like to try to make sense out of the countless “somethings” that made no sense.
And my physician – if armed with the facts we know today about alcohol misuse, secondhand drinking (second-hand impacts of drinking) and adverse childhood experiences (ACEs) – would have calmed me down and explained, “It’s real. It’s a problem. You’re not to blame, but you can improve the quality of your life.”
She could have then given me a simple handout that unlocked the secrets to what had been consuming my life and my health for decades. It would have explained alcohol use disorders, ACEs, SHD, and the extreme physical and emotional toll that repeated exposure to secondhand drinking causes because of the chronically activated fight-or-flight stress response system. It would have listed anonymous alcohol use assessments; key resources for further information; and programs that could have helped me – the family member of the loved one who drank too much.
We Need an SHD—ACEs Study
I first learned of the Adverse Childhood Experiences (ACE) Study in 2009. This study measured the impact of adverse childhood experiences* (ACEs) on a person’s health across a lifetime.
*Adverse Childhood Experiences (ACEs) are divided into three categories, neglect; abuse; and household challenges. They include physical, verbal, sexual abuse; physical, emotional neglect; and growing up with a relative with a substance use or mental disorder, to name a few.
This study drew the clear connection between exposure to ACEs and a person’s physical and mental health across their lifetime. To say the ACE Study rocked my world is to put it mildly. Here was the something that explained to me the previously inexplicable.
I now understood that exposure to my loved one’s drinking behaviors (SHD) most likely had the biggest impact on my ACEs. Not only that, but my other alcohol misusing loved ones had experienced their own ACEs, most likely as a result of their exposure to SHD. In other words, untreated SHD became untreated ACEs because none of us understood that alcohol misuse didn’t just affect the drinker’s health. It affected the health of non-drinkers (non-alcohol misusers). I shared some of my realizations in my earlier articles, When ACEs are Rooted in Secondhand Drinking and When Recovering From ACEs is Recovering from Secondhand Drinking and Visa Versa.
The parallel between exposure to alcohol misuse (drinking behaviors) and secondhand drinking health consequences and exposure to a person’s cigarette smoke and secondhand smoking health consequences became obvious to me.
Until society understood that secondhand cigarette smoke was extremely harmful to the health of the non-smoker, we tolerated people’s smoking in our cars, homes, airplanes, restaurants, and other public places. Prior to secondhand smoking health implications research, many pediatricians didn’t ask a child presenting with asthma if there was a smoker in their house. Instead the child was treated for asthma but returned to a secondhand smoking environment that only exacerbated their symptoms.
Similarly, as shared in my story of my 2012 lecture and still true today, until society understands a person’s alcohol misuse is extremely harmful to the health of the non-drinker (non-alcohol misusers), we will continue to tolerate a person’s drinking behaviors. We will continue to treat the presenting health symptom(s) but not the root cause, namely secondhand drinking related stress. And just as the secondhand smoking prevention efforts were not about preventing a smoker's right to smoke, neither is a secondhand drinking prevention effort about preventing a drinker's right to drink. Both are about not tolerating the second-hand effects on others.
Which brings me back to my premise. We need a study that provides an understanding of the physical, emotional, and quality-of-life impacts across a person's lifetime caused by exposure to secondhand drinking. We need a study that will provide the data necessary for health care professionals and professionals in related fields to understand the importance of querying their patients (clients) about alcohol misuse in the family. The study could be something along the lines of:
- Does a family member or close friend in your life drink alcohol?
- If yes, do you see or experience any of the following behavioral changes when they drink (provide examples of behavioral changes, aka drinking behaviors, with a graded scale for each: 1 = never and 5 = very often)?
- Are you experiencing (or have you experienced) any of the following physical or emotional health or quality of life conditions? (list would consist of an expansion of the stress-outcomes shared above, with a graded scale for each: 1 = never and 5 = very often).
This study would document outcomes for exposure to SHD in a manner similar to the ACE Study’s documentation of outcomes for exposure to adverse childhood experiences.
Indeed, there are many causes of ACEs unrelated to alcohol misuse, but the population of people dealing with SHD—ACEs is likely the single largest. Addressing the consequences in this population with a study like that outlined above could:
- Change the lives of the 90 million Americans affected by SHD, improving their physical and emotional health and quality of life by offering education and better prevention and treatment protocols
- Help us prevent ACEs for the one in four children who live in families with a parent addicted to alcohol (National Association for Children of Alcoholics (NACoA))
- Empower the medical and related professional communities’ screening for alcohol misuse in a patient/client’s sphere of influence, thereby screening for SHD | ACEs and, ultimately, helping their patients/clients treat the root cause of their health conditions and not just the symptoms
- Empowers each of us to change the dialogue and free ourselves from tolerating drinking behaviors (secondhand drinking) the same way we changed the dialogue around smoking and no longer tolerate secondhand smoking
- Educate society about alcohol misuse in general, which could do for those who misuse alcohol what the1964 Surgeon General’s Report on Smoking and Health did for those who smoked. The numbers of Americans who smoke cigarettes dropped to 15% in 2015 from 42% in 1964.
Related Studies:
For greater detail and other perspectives on SHD, I’m sharing these relatively recent studies / reports on second-hand effects of drinking:
Parental Drinking and Adverse Outcomes in Children: A Scoping Review of Cohort Studies
The Effects of Maternal Alcohol Use Disorders on Childhood Relationships and Mental Health
Global Research on Alcohol's Harm to Others
Facing Addiction in America, The Surgeon General’s Report on Alcohol, Drugs, and Health, 2016


Comments (5)